


Background
Mogamulizumab, an anti-CCR4 monoclonal antibody, is currently registered in the treatment of primary cutaneous T-cell lymphomas (Mycosis Fungoides and Sézary Syndrome). Its approval was based on the MAVORIC phase III trial, showing significantly improved progression-free survival compared with vorinostat. Drug-induced eruptions are reported as “very common” in the Summary of Product Characteristics (SmPC), but with no mention of ulceronecrotic evolution of skin lesions. We hereby report a case of severe ulceronecrotic evolution occurring during mogamulizumab in a patient with primary cutaneous peripheral T-cell lymphoma not otherwise specified (pcPTCL-NOS).
Objectives
To report a severe and previously undescribed ulceronecrotic evolution of cutaneous lymphoma lesions under mogamulizumab and to discuss potential mechanisms and pharmacovigilance signals.
Methods
A 55-year-old man was followed for nodular skin lesions of vascular appearance, predominantly affecting the lower limbs, evolving over several years without extracutaneous involvement. Histology repeatedly showed an atypical CD3+CD4+CD7- CD30- lymphocytic infiltrate with a dominant cutaneous T-cell clone and vascular component, consistent with pcPTCL-NOS. Multiple systemic therapies were administered sequentially (methotrexate, liposomal pegylated doxorubicin, pegylated interferon, bendamustine) with limited efficacy or significant toxicity. Mogamulizumab was introduced as fifth-line therapy (1 mg/kg weekly ×4, then every 2 weeks) based on CCR4 expression.
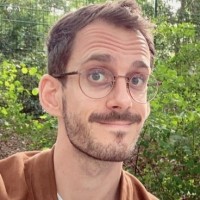
 Fig. 1. Tumoural lesions at initiation of mogamulizumab.
Fig. 1. Tumoural lesions at initiation of mogamulizumab.
Results
From day 3 after the first infusion, some nodules evolved toward painful ulceronecrotic lesions, while others remained stable or progressed. No systemic symptoms were observed. The condition worsened over weeks, leading to discontinuation after 8 infusions. Two months later, ulcerations persisted, some requiring skin grafting. Subsequent BV-CHP therapy led to progressive re-epithelialization and tumour flattening.
 Fig. 2. Ulceronecrotic evolution 6 weeks after last infusion.
Fig. 2. Ulceronecrotic evolution 6 weeks after last infusion.
Conclusion
Mogamulizumab-associated rashes are usually benign and non-necrotic. However, this case suggests a rare but severe ulceronecrotic evolution. Pharmacovigilance data (VigiBase) identify similar events, although causality remains difficult to establish. Possible mechanisms include immune dysregulation via T-reg depletion, autoantibody formation, or direct cytotoxicity in CCR4-expressing lesions. Close and prolonged clinical monitoring is essential in such patients.
As with any pharmacovigilance database, establishing a causal relationship between a reported adverse event and a suspected drug remains challenging. The conclusions derived from VigiBase do not represent the opinions of the WHO or affiliated institutions.
 Quentin Samaran
Quentin Samaran